Safety and efficacy of Tryngolza▼(olezarsen) were evaluated in adults with familial chylomicronemia syndrome (FCS) in the Balance trial: a randomised, placebo-controlled, double-blind phase 3 clinical trial1,2
The pivotal Balance trial1,2
Participants were randomised to receive olezarsen 80 mg (Tryngolza), olezarsen 50 mg* or placebo once every 4 weeks for 12 months1,2
*Olezarsen 50 mg is not an approved dosing regimen for FCS.1

The Balance study population was reflective of genetically confirmed FCS patients with severe disease1,2
The only Phase 3 pivotal trial that restricted enrolment to FCS patients with a genetically caused deficit of LPL activity1-4
In Tryngolza 80 mg treated patients (n=22):†
- 77% had a history of acute pancreatitis in the last 10 years, with 4.8 mean episodes per person (vs. 65% and 6.6 mean episodes per person in the placebo group)1,2
- Mean triglyceride level was 2613 mg/dL (vs. 2596 mg/dL in the placebo group)1,2
36% of Tryngolza and 43% of placebo group patients had received previous treatment with volanesorsen at baseline2
† Olezarsen 50 mg data are not presented as this is not an approved dosing regimen for FCS.1
Participant demographic and baseline characteristics were generally similar across treatment groups*1,2
Participants were generally representative of the FCS population.2
Across all treatment groups, most participants were on stable background lipid-lowering therapy, such as
statins, omega-3 fatty acids or fibrates.1,2
| Baseline characteristic2 | Tryngolza (n=22)2 | Placebo (n=23)2 |
| Body mass index (kg/m2; mean±SD) | 25.1±6.0 | 24.2±4.1 |
| History of acute pancreatitis in the prior 10 years | 17 (77%) | 15 (65%) |
| Type 1 or 2 diabetes | 7 (32%) | 6 (26%) |
| Hypertension | 4 (18%) | 6 (26%) |
| Triglyceride level (mg/dL; mean±SD) | 2613±1499 | 2596±1256 |
| apoC-III level (mg/dL; mean±SD) | 27.5±11.6 | 27.7±11.7 |
| Non–HDL cholesterol level (mg/dL; mean±SD) | 262.9±100.4 | 271.3±113.3 |
| Concomitant medications — no. (%) | ||
| Statin | 5 (23) | 7 (30) |
| Omega-3 fatty acid | 12 (55) | 7 (30) |
| Fibrate | 11 (50) | 11 (48) |
| Other lipid-lowering agent | 3 (14) | 3 (13) |
*Abbreviated baseline characteristics table.2
apoC-III = apolipoprotein C-III; HDL = high-density lipoprotein; SD = standard deviation
Trial inclusion criteria included:2,5
- Fasting TG levels ≥ 880 mg/dL
- Genetically identified FCS based on variants in genes known to cause complete or partial deficiency in LPL function.* Participants with indeterminate genetic test results were further assessed for (likelihood of) genetic confirmation of FCS by subject matter expert (using additional bioinformatic evaluation and research registry data)
- If participants were not already maintaining a low-fat diet, they undertook a ≥ 2-week dietary run-in period of ≤ 20 g fat per day

Primary endpoint (in order of hierarchy):
Mean percent change in fasting TG with olezarsen 80 mg (Tryngolza) or 50 mg from baseline to Month 6† compared with placebo2
Select secondary endpoints:
- Mean percent change in fasting TG with olezarsen 80 mg from baseline to Month 12‡ compared with placebo2,5
- Comparison of adjudicated acute pancreatitis event rate of pooled Tryngolza 80 mg and olezarsen 50 mg treatment groups vs placebo during the treatment period2,5
- Comparison of percent change in fasting apolipoprotein B-48 (apoB-48) from baseline to Month 6 of Tryngolza 80 mg vs pooled placebo2,5
- Comparison of percent change in fasting non-high density lipoprotein cholesterol from baseline to Month 6 of Tryngolza 80 mg vs pooled placebo2,5
*Variants were LPL, APOA5, GPIHBP1, LMF1 or APOC2.2
†Average of Weeks 23, 25 and 27.1,2
‡Average of Weeks 51 and 53.5
APOA5 = apolipoprotein A5; APOC2 = apolipoprotein C2; GPIHBP1 = glycosylphosphatidylinositol-anchored
high-density lipoprotein binding protein 1; LMF1 = lipase maturation factor 1; LPL = lipoprotein lipase.
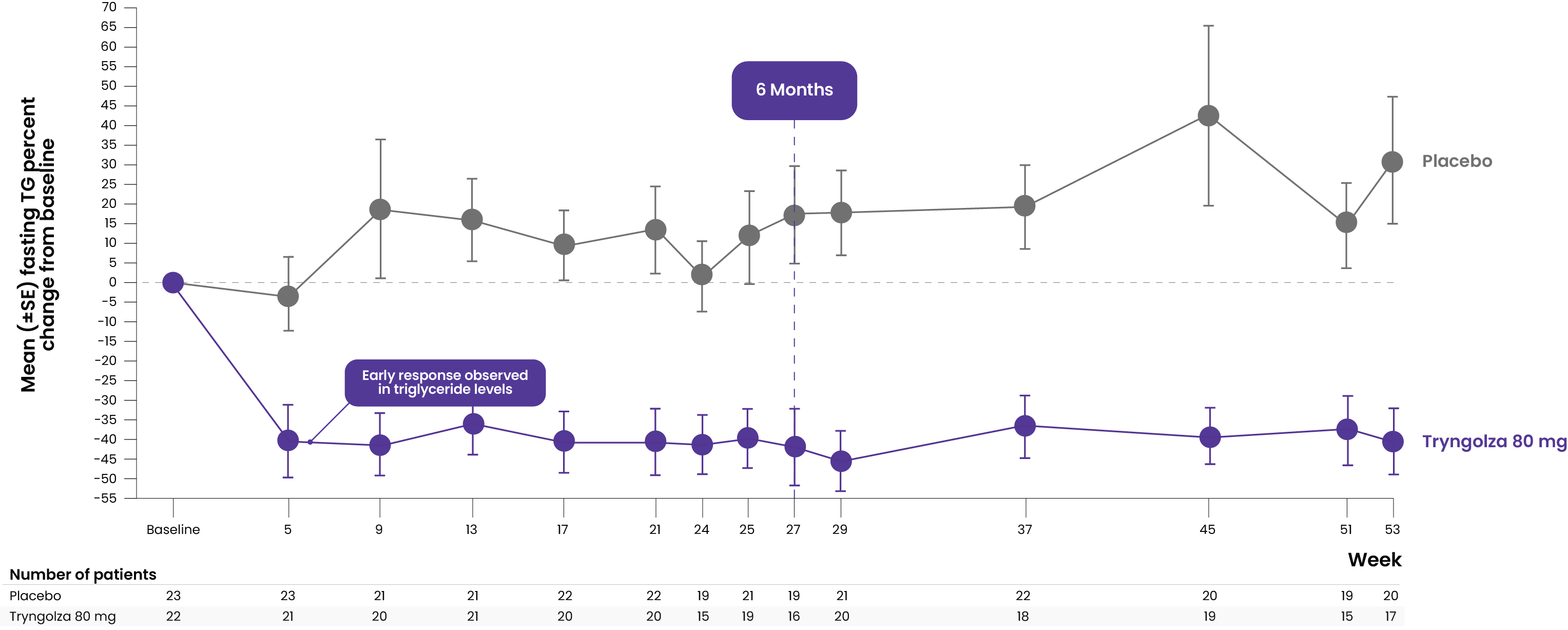
Significant reduction in triglyceride levels helps support treatment goal of reduced acute pancreatitis incidence2,6
Significantly reduced fasting TG levels at Month 6 vs placebo2
LSM % change (95% CI) from baseline, placebo-adjusted



Second primary outcome of change in TG levels with olezarsen 50 mg at 6 months from baseline vs placebo did not reach significance (LSM -22.4% [95% CI, -47.2 to 2.5]; P=0.08). Therefore, all secondary outcomes are non-confirmatory


Numerical reduction in AP events over 12 months — 2 episodes overall in olezarsen groups (levent each in 50 mg and 80 mg arms) vs. 11 episodes in the placebo group.
Mean rate ratio: [pooled Tryngolza 80 mg and olezarsen 50 mg groups vs placebo]: 0.12 (95% CI, 0.02 to 0.66) (non-confirmatory)
*Average of Weeks 23, 25 and 27. Tryngolza 80 mg patients had high baseline mean TG of 2613 mg/dL, 77% with prior pancreatitis.2,5
†Average of Weeks 51 and 53.5
‡All secondary endpoints were non-confirmatory. The 95% confidence intervals for the secondary endpoints were not adjusted for multiplicity, and the results should not be interpreted as hypothesis tests. Olezarsen 50 mg is not an approved dosing regimen for FCS.1,2


Reduced TG level led to an 88% reduction in AP incidence compared to placebo*†2
AP incidence over 1 year (secondary endpoint)


Delayed onset to first pancreatitis event by 348 days with Tryngolza 80 mg compared to placebo*†5
Time to first event

*Numerical reduction in AP events over 12 months – 2 episodes overall (1 event each in olezarsen 50 mg and Tryngolza 80 mg arms) vs. 11 episodes in the placebo group. Mean rate ratio [pooled olezarsen groups vs placebo]: 0.12 (95% CI, 0.02 to 0.66; nominally significant). Secondary endpoints were prespecified and rank prioritised to be analysed in hierarchical order. Given the second primary endpoint (difference in the percent change in fasting TG level from baseline to 6 months in the 50 mg olezarsen group compared with placebo) was not statistically significant, all secondary endpoints were considered exploratory and presented as least-squares mean changes with the 95% confidence intervals, mean rate ratios with the 95% confidence intervals, or percentages. The 95% confidence intervals for the secondary endpoints were not adjusted for multiplicity, and the results should not be interpreted as hypothesis tests. Olezarsen 50 mg is not an approved dosing regimen for FCS.1,2
†Time to first patient in placebo group and first patient in Tryngolza 80 mg group to experience an AP event. At baseline, 77%, 71% and 65% of patients had a history of AP and experienced a mean of 4.8, 4.1 and 6.6 episodes of AP per patient in the previous 10 years in the Tryngolza 80 mg, olezarsen 50 mg and placebo groups, respectively.2

Tryngolza had a well-tolerated safety profile in participants with familial chylomicronemia syndrome (FCS)1,2
The safety of Tryngolza was evaluated in 43 participants who received at least 1 dose of treatment; 23 participants in the Balance trial received placebo*1,2
- Mean platelet counts remained within normal limits during the study, and no participant treated with Tryngolza with FCS had a platelet count <50,000/mm3. There were no major bleeding events associated with a low platelet count.1,2
| Adverse events that occurred during the treatment period – no. of patients (% of patients)2 | ||
| Tryngolza 80 mg (N=22) | Placebo (N=23) | |
| Any adverse event | 19 (86%) | 22 (96%) |
| Serious adverse events | 3 (14%) | 9 (39%) |
| Adverse events leading to discontinuation† | 2 (9%) | 0 |
Abbreviated adverse events table.2
- Most common adverse events: coronavirus disease, abdominal pain, diarrhoea (none of which occurred more frequently among patients who received either dose of olezarsen than those who received placebo); patients who received olezarsen did not experience any serious adverse events related to the trial drug2
- No imbalances among the three Balance trial groups with respect to liver, renal or platelet laboratory variables; mild injection-site reactions were more common with olezarsen than with placebo2
- †Reported adverse events that led to treatment discontinuation included diarrhoea, vomiting, chest discomfort, chills, myalgia, trismus and flushing1,2
*The safety of Tryngolza was evaluated in 66 participants with FCS enrolled in the Balance trial. In this trial, 43 participants received at least one dose of Tryngolza, 50 mg (n = 21) or 80 mg (n = 22), and 23 participants received placebo. Olezarsen 50 mg is not an approved dosing regimen for FCS.1,2
References
- Tryngolza EU Summary of Product Characteristics. December 2025.
- Stroes ESG, et al. N Engl J Med. 2024;390(19):1781–1792.
- Witztum JL, et al. N Engl J Med. 2019;381:531–542.
- Watts GF, et al. N Engl J Med. 2025;392:127–137.
- Stroes ESG, et al. N Engl J Med. 2024;390(19) (supplementary appendix):1781–1792.
- Javed F, et al. J Clin Lipid. 2025;19:382–403.
Tryngolza▼(olezarsen) is indicated as an adjunct to diet in adult patients for the treatment of genetically confirmed familial chylomicronemia syndrome (FCS).
▼This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. See section 4.8 of the SmPC for how to report adverse reactions.
Healthcare professionals should report any suspected adverse reactions via their national pharmacovigilance reporting system. Suspected adverse reactions should also be reported to Sobi via email at [email protected].
This material is intended for an international audience of healthcare professionals and is based on the Tryngolza Summary of Product Characteristics (SmPC) approved for use in the European Economic Area (EEA). SmPC/Prescribing information, product availability, and pricing/reimbursement conditions may vary by country. Before prescribing, always refer to locally approved SmPC and/or prescribing information.
The Sobi Scientific Information Department is at your disposal for any additional information: [email protected].
© 2026 Sobi – Swedish Orphan Biovitrum AB (publ), SE-112 76 Stockholm, Sweden. www.sobi.com/en
All rights reserved.
SOBI is a trademark of Swedish Orphan Biovitrum AB (publ).
TRYNGOLZA is a registered trademark of Arexis AB, a Sobi company, and Ionis Pharmaceuticals, Inc.
TRYNGOLZA (olezarsen) – Discovered by Ionis Pharmaceuticals, Inc.
All third-party trademarks are the property of their respective owners.