VALIANT:2
The largest and broadest Phase 3 study in patients >12 years with native or recurrent C3G or primary IC-MPGN2,8
The trial population was aligned with the known demographics of real-world patients with C3G.2,9
Valiant Study Design
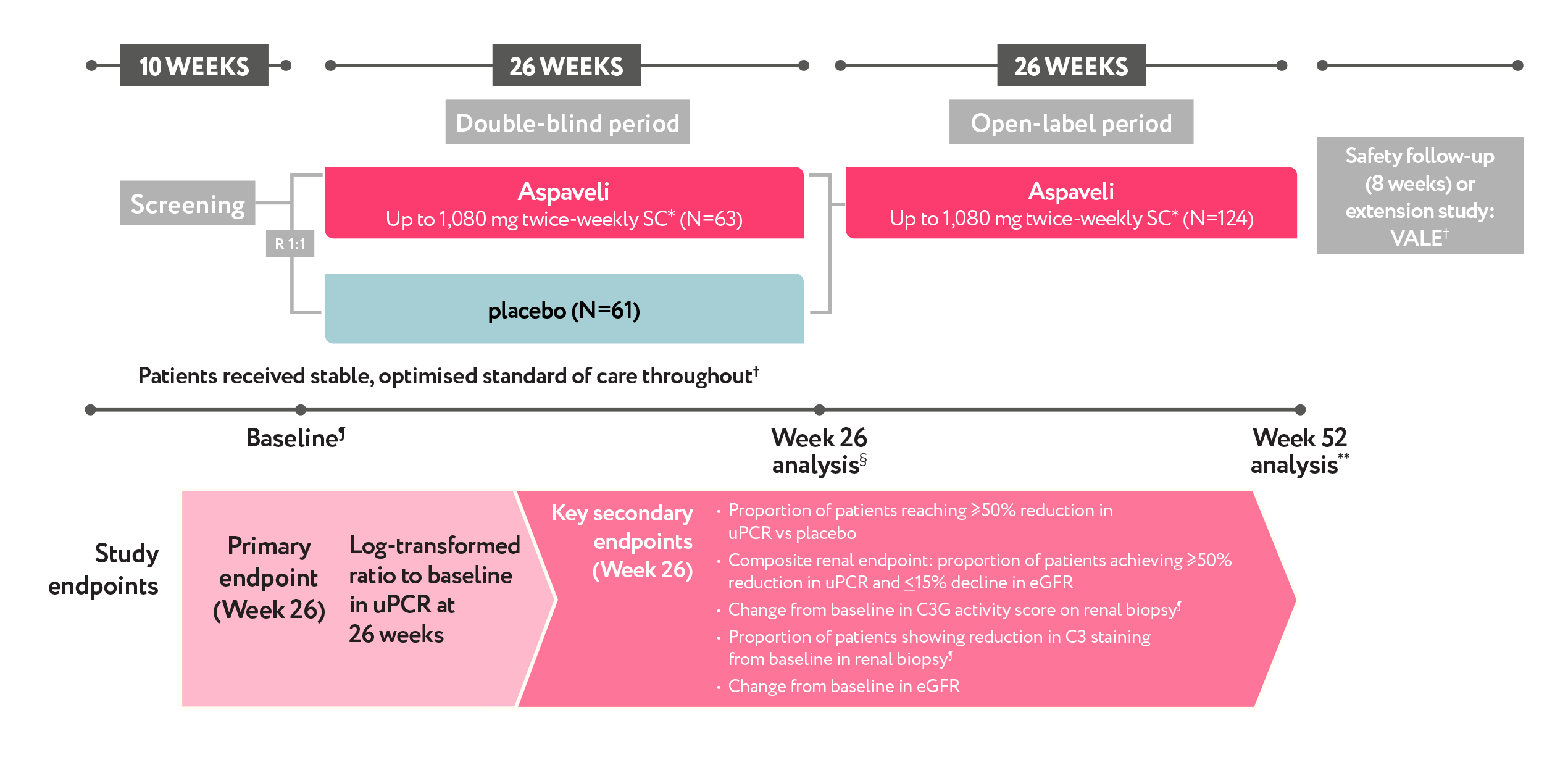
VALIANT: The largest and broadest Phase 3 study in patients ≥12 years with native or recurrent C3G or primary IC-MPGN1,2,11
STUDY DESIGN2
Relative reduction†† (95% CI), Aspaveli® vs placebo
68.1%
(57.3, 76.2)
p<0.001¶¶2
Maintained a consistent proteinuria reduction over 52 weeks10
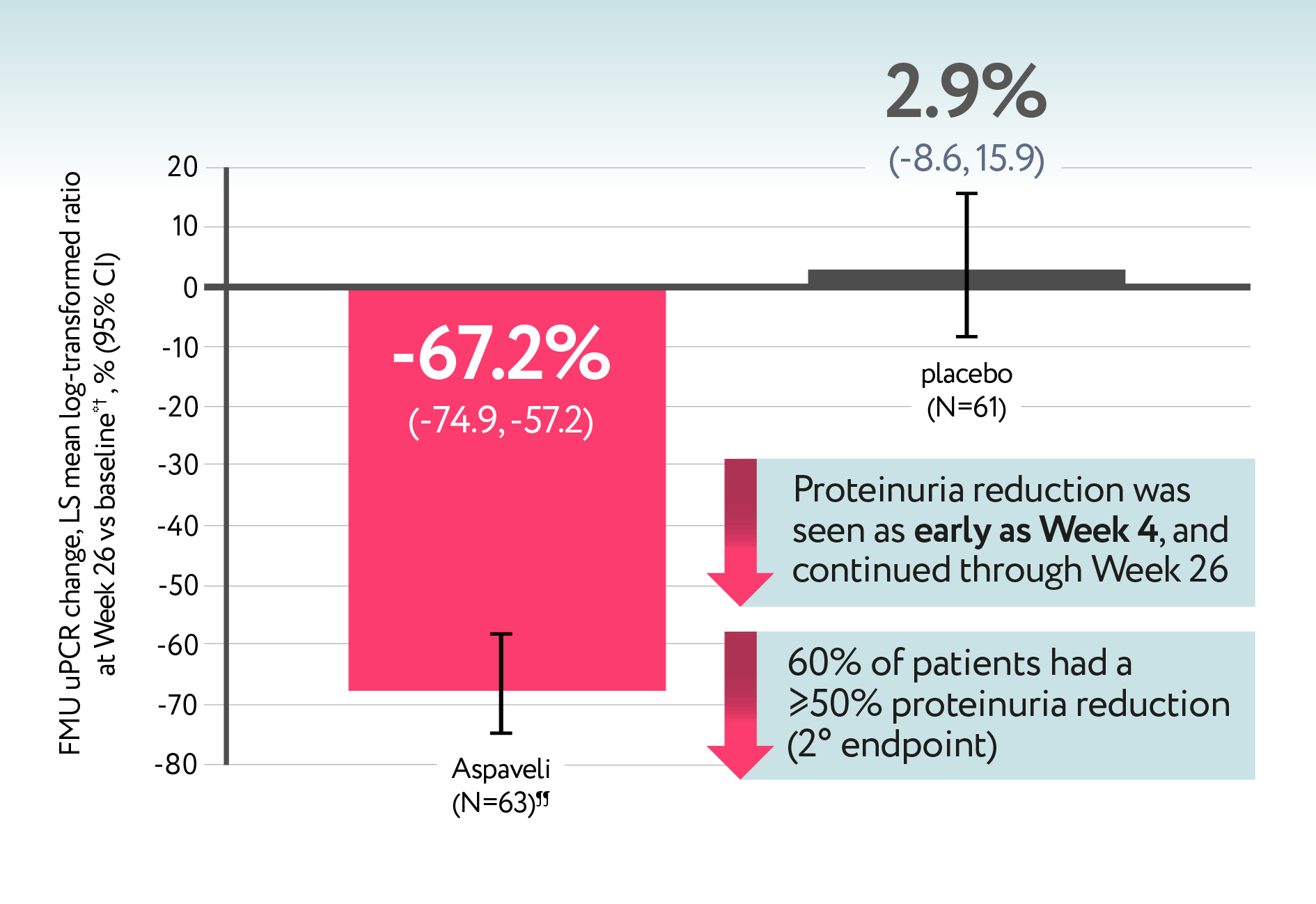
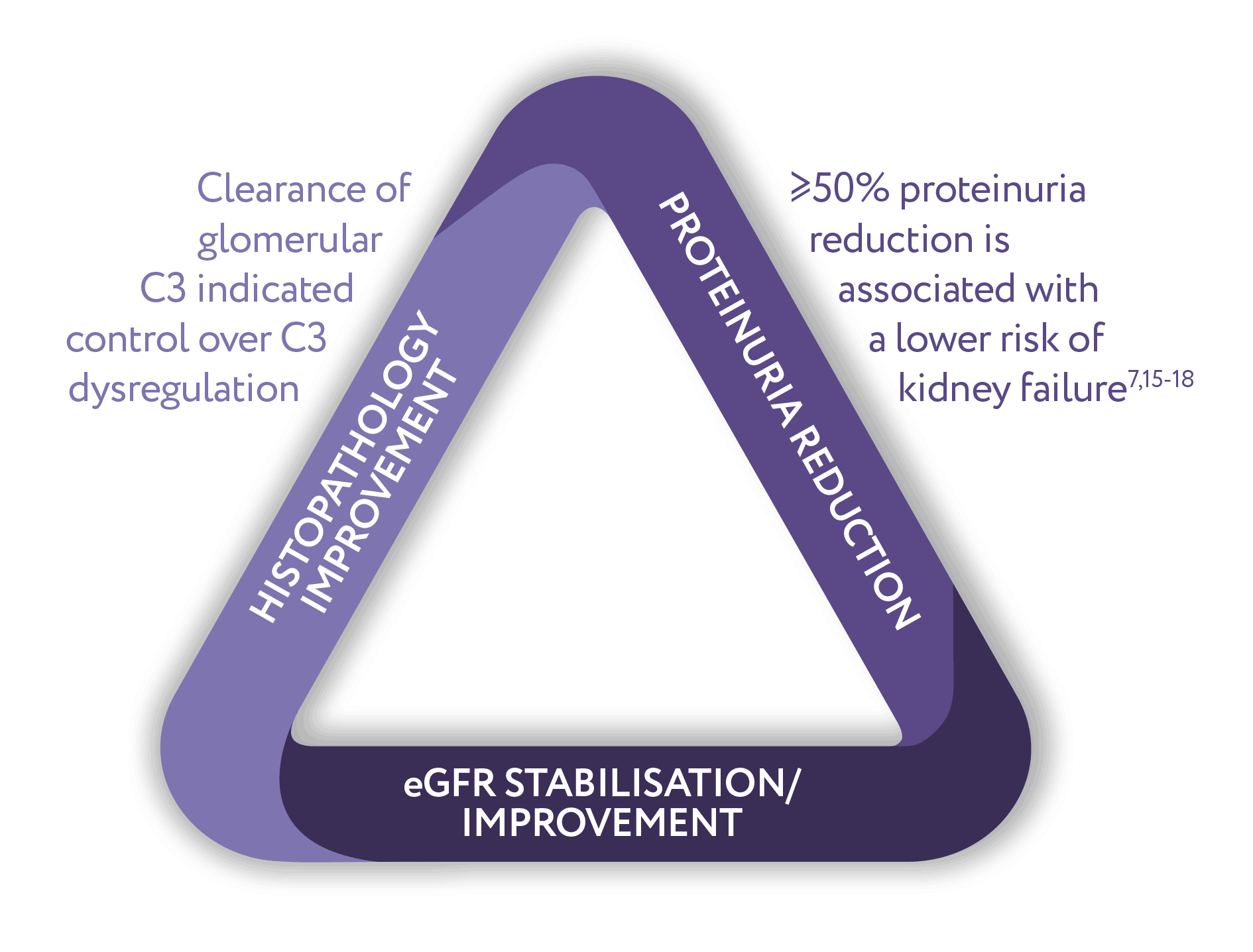
Patients were 31x more likely to achieve a >50% reduction with Aspaveli® vs placebo.2,8
In a post-hoc analysis 51% of Aspaveli®-treated patients achieved <1g/g proteinuria after just 26 weeks.2,9
Proteinuria reduction was consistent across the VALIANT study populations and patient types*2
Explore a possible future treatment algorithm for C3G and primary IC-MPGN
Proteinuria reduction in pre-specified subgroups
| Proteinuria reduction in pre-specified subgroups2 |
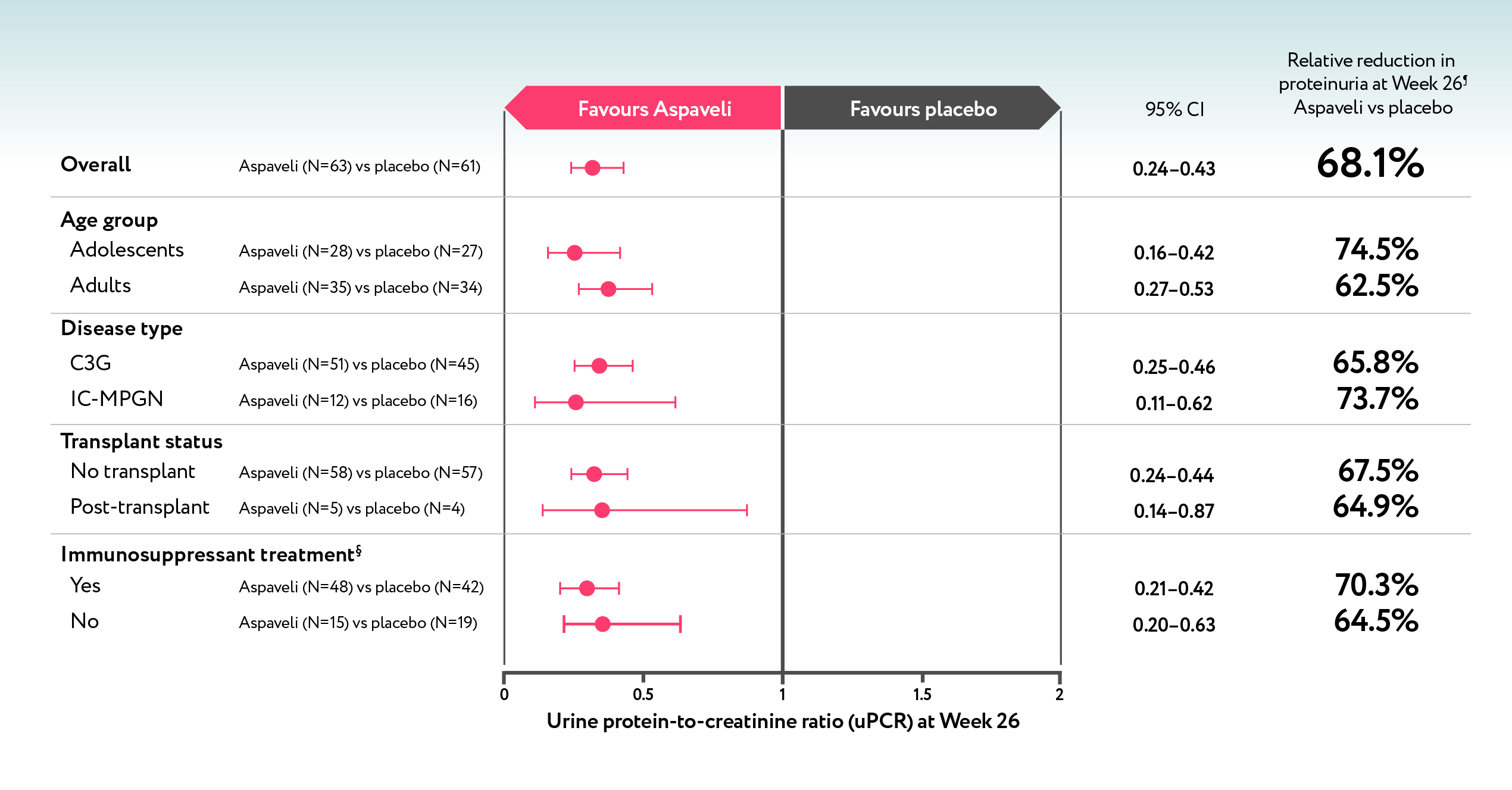
Intent-to-treat population (all randomised patients).
Key secondary endpoint
An overall relative eGFR +6.3 mL/min/1,73m2 (95% CI: 0.5-12.1) eGFR relative change from baseline vs. placebo2
Aspaveli stabilised renal function, while eGFR continued to decline with placebo2
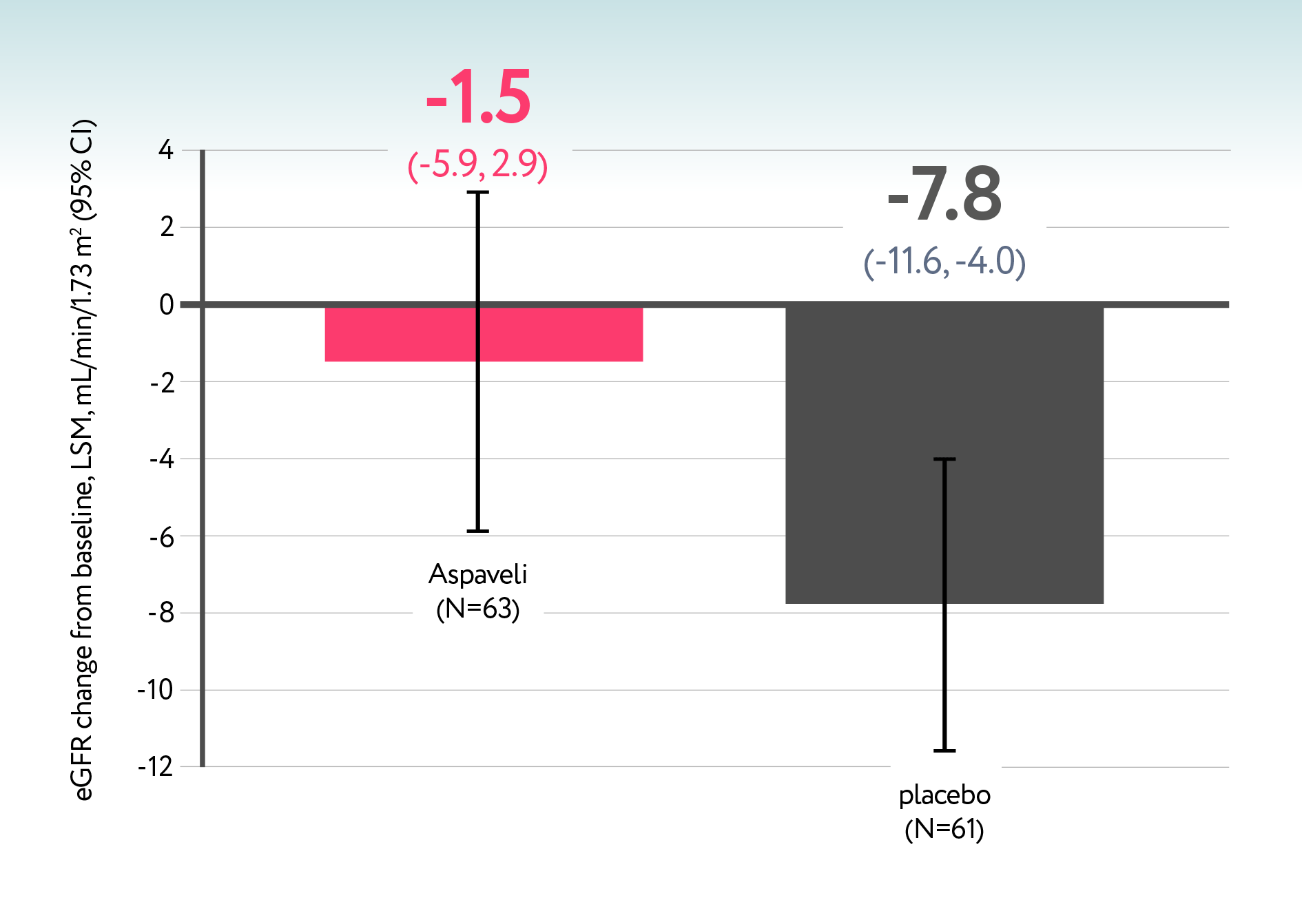
Stabilised renal function
across study subgroups2,8,10-14
eGFR remained stable over 52 weeks with Aspaveli, while patients switching from placebo showed stabilization after entering the open-label Aspaveli period10
71.4%
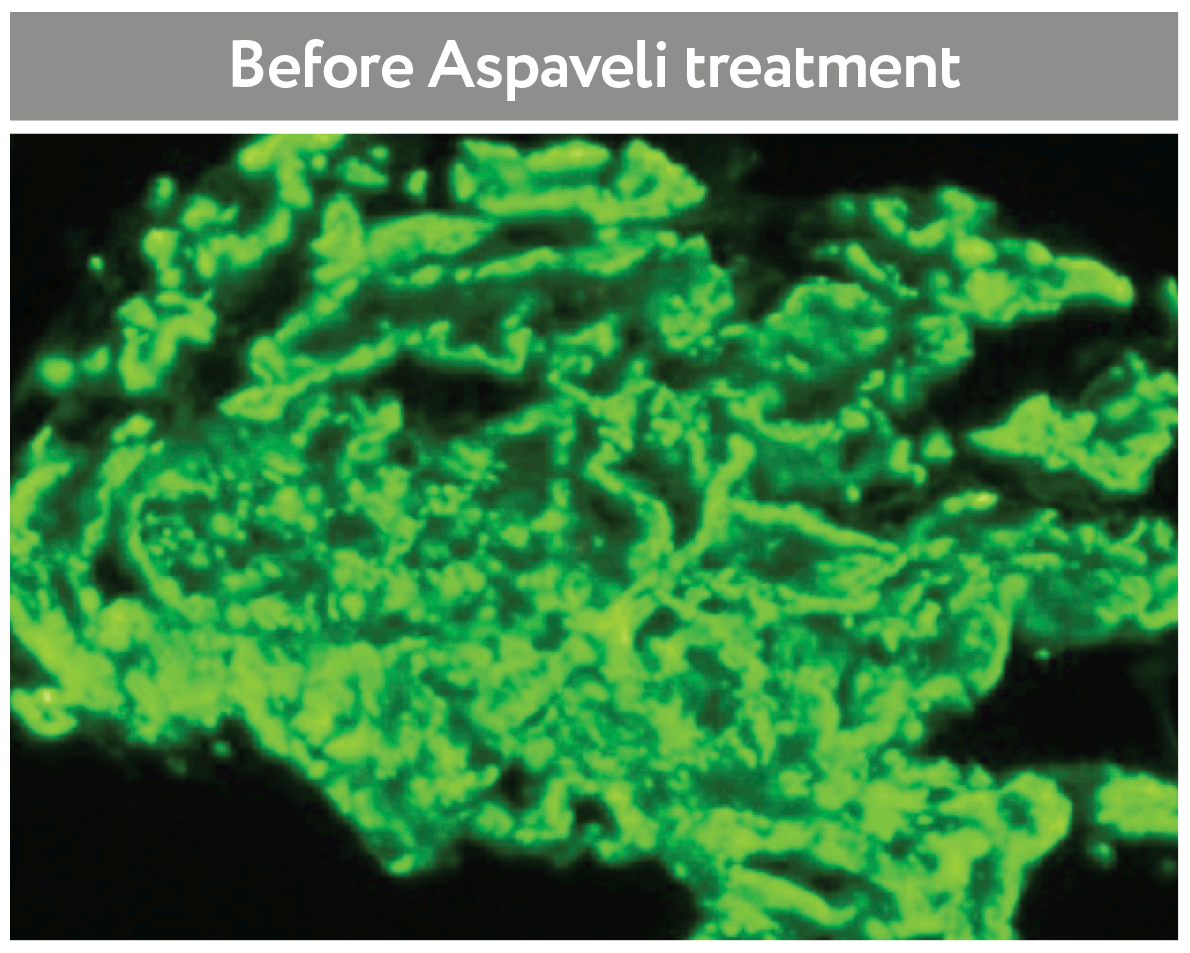
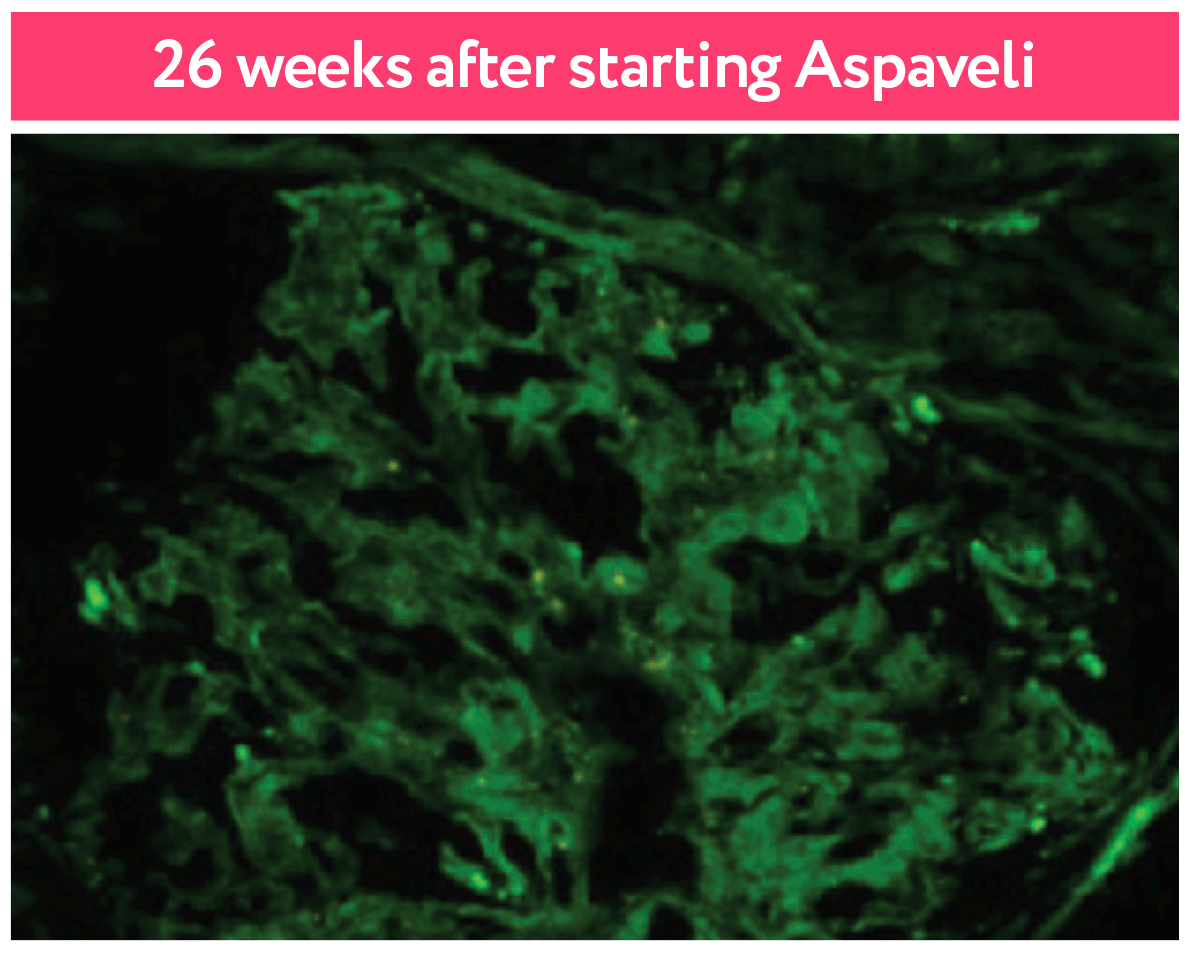
(25/35) of Aspaveli®-treated patients achieved 0 intensity staining2
Renal biopsies showed 74% (26/35) of Aspaveli®-treated patients achieved a reduction in staining (≥2 point improvement on the 0–3 scale) by week 26***2,9
Zero intensity staining was also achieved by 100% (4/4)†††12 of transplant patients and 65.4% (17/26) of IS and 88.9% (8/9) of no-IS patients treated with Aspaveli®14
Downloadable documents
EMA indication:
ASPAVELI® is indicated for the treatment of adult and adolescent patients aged 12 to 17 years with C3 glomerulopathy (C3G) or primary immune-complex membranoproliferative glomerulonephritis (IC-MPGN) in combination with a renin-angiotensin system (RAS) inhibitor, unless RAS inhibitor treatment is not tolerated or contraindicated.1
| For the full EMA Aspaveli SmPC, please click here |
▼This medicine is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions via their national pharmacovigilance reporting system. Suspected adverse reactions should also be reported to Sobi via email at [email protected].
Abbreviations
C3, complement 3; C3G, C3 glomerulopathy; CI, confidence interval; eGFR, estimated glomerular filtration rate; FMU, first-morning spot urine; IC-MPGN, immune complex-mediated membranoproliferative glomerulonephritis; KHI, Kidney Health Initiative; LSM, least squares mean; RAS, renin-angiotensin system; uPCR, urine protein-to-creatinine ratio.
Footnotes
* All adults and adolescents weighing ≥50 kg self-administered 1,080 mg/20 mL. Adolescent patients weighing 30–34 kg received 540 mg/10 mL for the first 2 doses, then 648 mg/12 mL. Adolescent patients weighing 35–49 kg received 648 mg/12 mL for the first dose, then 810 mg/15 mL.8 † Stable, optimised antiproteinuric regimens: ACEis, ARBs, SGLT2is, MMF, and corticosteroids (prednisone <20 mg/dayor equivalent) were permitted in both treatment arms.2 ‡ Adult baseline biopsies are those performed during screening to confirm diagnosis/eligibility, or historical biopsies conducted within 28 weeks of study randomisation. Baseline biopsies will not be required for adolescent patients if an adequate historical biopsy conducted at any time is available to confirm diagnosis.2 ¶ The Week 26 biopsy is only required for adult patients to advance to the OLE period but is not required for adolescent patients who may advance to the OLE period without a biopsy.2,8 § The Week 52 biopsy is optional for all patients.10 ** Participants entering the long-term extension study will not complete the follow-up period.8 ††Using an equal-weighted average from FMU over Weeks 24, 25 and 26.2 ‡‡ Percentages calculated by converting the ratio of geometric means to percentages.2 ¶¶ p<0.001. Intent-to-treat population (all randomised patients).2 §§ Renal biopsies from a Aspaveli-treated C3G native kidney patient.2 *** A reduction in staining was defined as ≥2 point improvement on the 0–3 scale of the C3G histologic index activity score.2,8,9 ††† Evaluable baseline and Week 26 renal biopsies were only available for 4 out of 5 transplanted patients.2
References
Aspaveli EMA Summary of product characteristics. Swedish Orphan Biovitrum AB (publ) January 2026.
Fakhouri F, et al. N Engl J Med 2025;393:2210–20.
Simon-Tillaux N, et al. Presented at American Society of Nephrology Kidney Week 2019, Washington DC, USA; 7–9 November. Poster SA-PO609.
Bomback AS, et al. Kidney Int Rep 2025;10:87–98.
Dixon B, et al. Kidney Int Rep 2023;8:2284–93.
Hoy SM. Drugs 2021;81:1423–30.
Nester CM, et al. Clin J Am Soc Nephrol 2024;19:1201–8.
Fakhouri F, et al. N Engl J Med 2025;393:2210–20 (Supplementary appendix).
Kavanagh D, et al. Kidney Int Rep. 2026;11(1):17–31.
Fakhouri F, et al. Abstract presented at ERA Congress 2025, Vienna, Austria; June 4–7 2025. Abstract 77.
Mastrangelo A, et al. Nephrol Dial Transplant. 2025;40(Suppl 3):gfaf116.019.
Oosterveld M, et al. Nephrol Dial Transplant. 2025;40(Suppl 3):gfaf116.0325.
Kavanagh D, et al. Nephrol Dial Transplant. 2025;40(Suppl 3):gfaf116.020.
Kavanagh D, et al. Presented at ERA Congress 2025, Vienna, Austria; 4–7 June 2025. Abstract 288.
Wong E, et al. Kidney Int Rep 2023;8(12):2754–64.
Masoud S, et al. Kidney Int 2025;108(3):455–69.
Caravaca-Fontán F, et al. Nephrol Dial Transplant 2022;37:1270–80.
Ghaddar M, et al. Clin J Am Soc Nephrol 2025;20(8):1119–31.